
Stroke Recovery Guide
Stroke [& Neurological] Recovery – Complete Guide to Healing After Brain Injury
Your complete stroke recovery guide: survivor story, exercises, neuroplasticity, emotional healing, tools, and hope for rebuilding life after brain injury.
Download our free printable recovery checklists designed to support different areas of stroke rehabilitation. Choose the Card most relevant to your needs and use it to track your progress at your own pace.
Physical Stroke Recovery Checklist
Track your daily physical rehabilitation activities, including mobility, balance, strength, and self-care tasks. This printable checklist helps you monitor progress and build consistency throughout your recovery.
Speech and Cognitive Recovery Checklist
Support your communication and cognitive recovery with exercises focused on speech, memory, concentration, and daily mental activities. Use this checklist to track improvements and identify areas that need extra attention.
Daily Wellbeing Recovery Checklist
Monitor nutrition, hydration, sleep, medication management, and healthy daily routines. This checklist helps you build habits that support your overall recovery and wellbeing.
Visual Recovery Checklist
Track activities that support visual rehabilitation, including eye exercises, reading practice, scanning tasks, and fatigue management. Use this checklist to make visual recovery progress easier to follow.
What Is a Stroke?
What Really Happens During a Stroke
Ischemic Stroke Animation:
A blood vessel becomes blocked or bursts
Oxygen stops reaching a part of your brain
Cells begin to die
Functions controlled by that area change instantly
Understanding the Three Main Types of Stroke
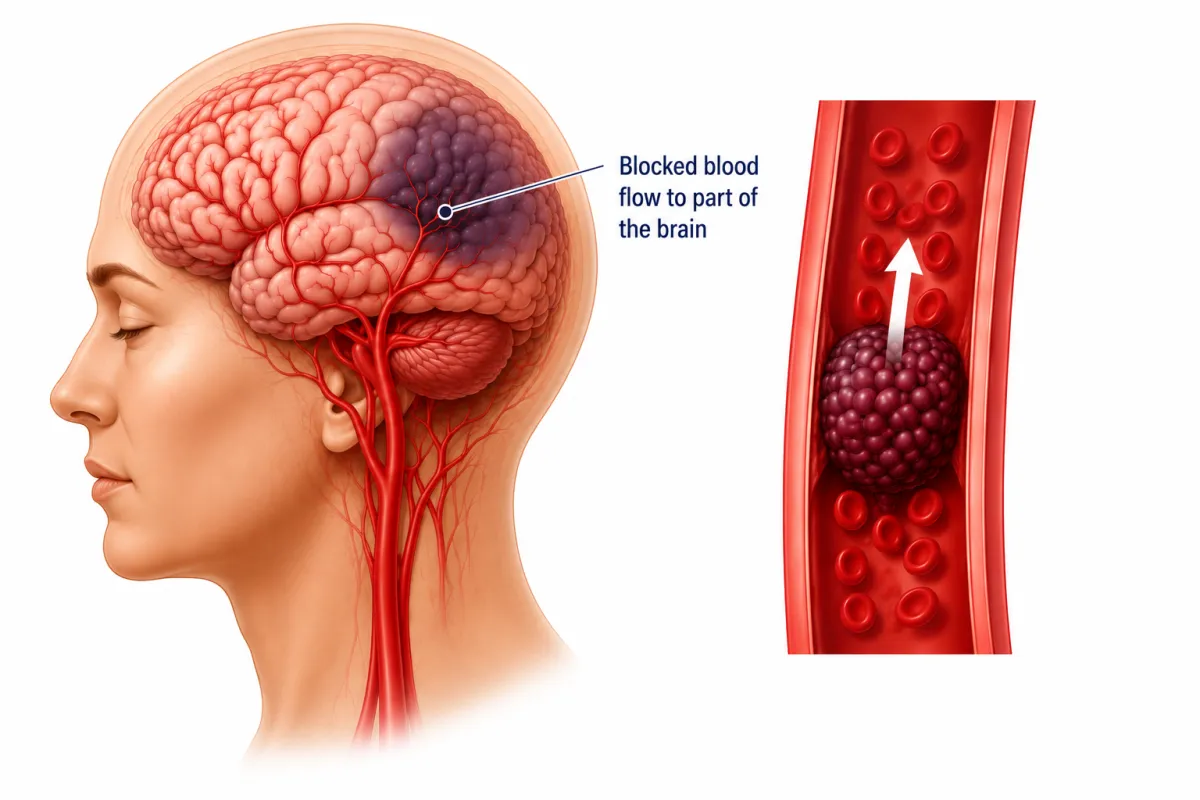
Ischaemic: blockage
An ischaemic stroke occurs when a blood vessel supplying the brain becomes blocked, usually by a blood clot or a build-up of plaque. This blockage stops oxygen-rich blood from reaching the affected area, causing brain cells to become stressed and begin to die within minutes. Because the brain depends on constant blood flow to function, even a small obstruction can disrupt movement, speech, memory, or other abilities controlled by that specific region. This is the most common type of stroke, accounting for the majority of cases, and early recognition and treatment are critical to reducing long-term damage.
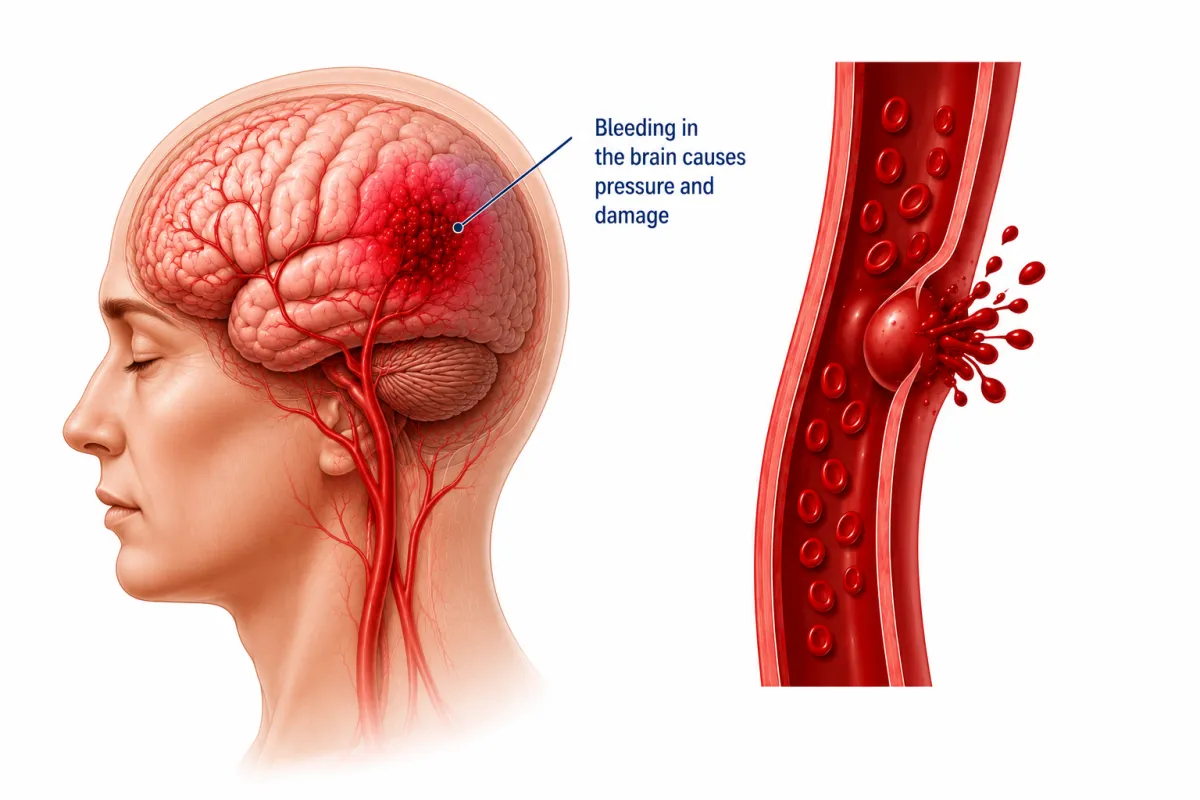
Haemorrhagic Stroke : Brain bleed
A haemorrhagic stroke happens when a blood vessel in the brain bursts, causing bleeding into or around the brain tissue. This sudden bleeding creates pressure that damages nearby brain cells and disrupts the normal flow of oxygen and nutrients. The affected area can no longer function properly because the accumulating blood irritates and compresses the brain. Haemorrhagic strokes are less common but often more severe, and they usually occur due to long-term high blood pressure, weakened vessel walls, or aneurysms. Early medical intervention is critical to control the bleeding and protect the brain from further injury.
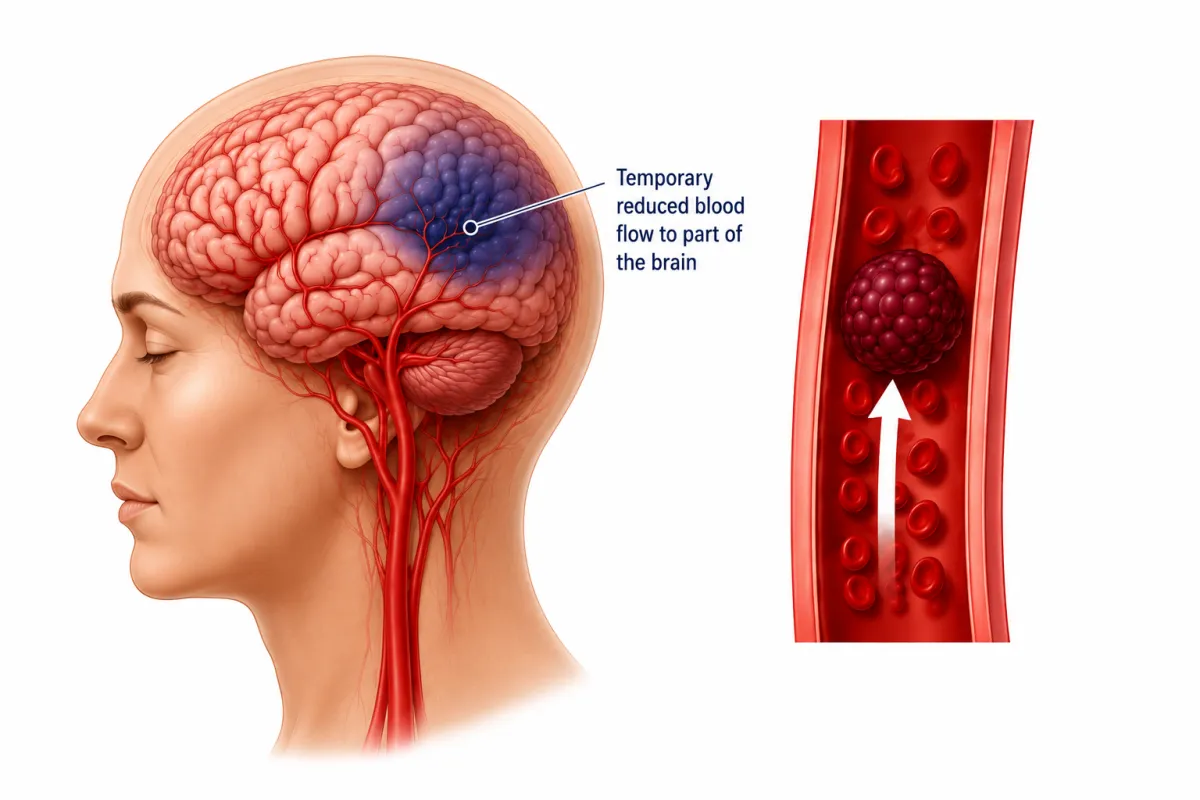
Temporary Clot - TIA
A Transient Ischaemic Attack (TIA) happens when a temporary clot briefly blocks blood flow to part of the brain. The symptoms look and feel like a stroke but disappear within minutes to hours because the blockage clears on its own. Even though the effects are short-lived, a TIA is a serious warning sign that a major stroke may follow. It’s the brain’s early alert system, giving a crucial opportunity to seek medical help, identify the cause, and start treatment to prevent a future, potentially life-changing stroke.
F.A.S.T. Stroke Guide — Act Immediately
The F.A.S.T. test is the quickest and most widely used way to recognise the most common and dangerous stroke symptoms. It focuses on signs that indicate a sudden interruption of blood flow to the brain and require immediate emergency treatment.
If any one of these signs is present, treat it as a medical emergency.

F — Face drooping
Ask the person to smile.
Look for:
One side of the face drooping or sagging
Numbness or weakness on one side of the face
An uneven or asymmetrical smile
Facial drooping occurs when the brain areas controlling facial muscles are not receiving enough oxygen.
A — Arm weakness
Ask the person to raise both arms at the same time.
Look for:
One arm drifting downward
Inability to lift one arm
Sudden weakness, heaviness, or numbness in one arm
Arm weakness is one of the most common stroke symptoms and often affects one side of the body.


S — Speech difficulty
Ask the person to repeat a simple sentence.
Listen for:
Slurred or garbled speech
Difficulty finding words
Trouble understanding what is being said
Speech changes indicate that the brain’s language or motor-speech centres may be under stress.
T — Time to call emergency services
If you observe any of the above signs — even if symptoms improve or disappear — call emergency services immediately.
Do not wait.
Do not drive yourself.
Do not assume it will pass.
Time lost is brain lost. Fast treatment can reduce long-term disability and save lives.

After F.A.S.T. Has Been Followed — Apply B.E.
These signs help identify strokes that may not present clearly with F.A.S.T. alone, particularly strokes affecting balance, vision, or the brainstem.

B — Balance problems
Watch for:
Sudden dizziness or vertigo
Loss of balance or coordination
Difficulty standing or walking straight
Sudden unexplained falls
Balance problems are common when stroke affects the cerebellum or brainstem and may appear without facial or arm weakness.
E — Eye or vision changes
If you observe any of the above signs — even if symptoms improve or disappear — call emergency services immediately.
Sudden vision loss in one or both eyes
Blurred or double vision
A curtain, shadow, or blind spot appearing
Sudden visual changes are a recognised stroke symptom and should always be reported to emergency responders.

Key Takeaway
Use F.A.S.T. first, then BE
When in Doubt — Act
You do not need all the signs for it to be a stroke.
You do not need certainty.
You only need one sudden neurological change.
Acting quickly:
Protects brain tissue
Improves recovery outcomes
Reduces long-term disability
Saves lives
My Stroke Survivor Story: From Paralysis to 96% Recovery

The Moment My Body Stopped — The Day My Stroke Began
That morning began like any other. I kissed my husband goodbye, dropped our little one at nursery, and settled into my home office under a bright, hopeful sky. I felt healthy, strong, full of dreams—but life, as I knew it, was about to change forever.
By the afternoon, I headed to the supermarket, picturing dinner, when something strange caught me mid-step. I was wearing only one shoe, having crossed rough, uneven ground without noticing. A cold wave of confusion swept over me. Then it hit—a sudden numbness on one side of my body, a weakness I had never felt before, and a searing, lightning-like pain shot through my head. The short walk to the store became impossible. I stumbled back to my car, desperate and terrified, not yet realizing I was experiencing the early signs of a major stroke.
Back at home, I tried to stand—and the world betrayed me. I collapsed, my left side completely unresponsive, as if my body had turned to stone. Every movement was a struggle; even the simplest act of reaching for something felt impossible. In that instant, life as I knew it had stopped. Independence, strength, and freedom—the things I had always taken for granted—were stripped away in a heartbeat. I was trapped in a body that no longer obeyed me, confronted with the terrifying reality of sudden stroke paralysis. Time slowed, fear surged, and the fragility of life became shockingly, painfully clear.
What I Felt After My Stroke — Fear, Confusion, and Paralysis
When the diagnosis came, fear swallowed me whole. Lying there, unable to feel my left side, I felt imprisoned in a body that had betrayed me. Each prick of the needle that brought no sensation was a cruel reminder that my independence, my strength, my freedom—all had been stolen in an instant. The reality of brain damage—my “brain attack”—was overwhelming. I was plunged into shock, disbelief, and confusion, struggling to comprehend how a single clot could disrupt the intricate network of neurons that had carried me through life.
The world around me felt unreal, as if the floor had shifted beneath my feet and I had been thrust into a nightmare I couldn’t escape. Fear hit like a tidal wave—cold, sharp, and impossible to ignore. It wrapped around my chest, squeezing my lungs until my heart hammered as though it might burst. My thoughts raced uncontrollably, tumbling through my mind like stones down a cliff, each one crashing into the next: What if I never move again? What if I can’t care for my child, my family, or myself? Will I ever walk, talk, or live the life I knew? Anxiety and dread rose in relentless waves, threatening to pull me under. it surged through me like a merciless tide, pounding my chest, knotting my stomach, and tightening every muscle in my body. Each breath came shallow and sharp, as if the air itself had thickened around me.

Physically, my body had become a stranger—paralyzed, weak. My feet, once reliable and strong, now lay there unresponsive and still, like a foreign object I could no longer command. Doctor! I cried, please, I need my f00t! I have a young child to care for.
Panic surged through me as I stared at it, my mind screaming in disbelief. I cried with each failed attempt to move my left limps. I stared at them, mourning the simple movements I had always taken for granted. Emotionally, I wrestled with a profound sense of loss—of my body, my abilities, and a part of myself. The helplessness was crushing, the isolation suffocating, and the experience utterly overwhelming. It was terrifying, disorienting, and impossible to escape.

The First Signs of Stroke Recovery — When Movement Began to Return
The first sparks of movement were almost miraculous, so small I almost missed them. My fingers twitched, a faint, trembling flutter, like tiny wings testing the air. I stared at them, disbelief and hope warring in my chest. Could this be real? Could my body, which had betrayed me, remember itself?
Then my hand lifted slightly, shakily, as if moving through thick syrup. Each motion sent a jolt of exhilaration through me—so small, yet so monumental. But my hand was hypersensitive to everything. I braced myself against the rough pebble-dash wall to stop from falling, and it felt as though I had pressed sharply against hundreds of broken shards of glass. Cold water felt like ice cutting into my skin, warm water burned, and steam from cooking scalded instantly. Every sensation was amplified, overwhelming, and painful. I had to reintroduce my hand to the feeling of different textures and temperatures, slowly and carefully, learning again what was safe, what was normal, and how to stop the constant pain. Each tiny movement became not only a physical triumph but a painstaking lesson in trusting my body and reconnecting with the world around me.
Learning to Walk Again After Stroke — Small Victories That Changed Everything
My foot soon followed, though my toes were the last to respond. Each movement was slow and heavy, my foot feeling weighted, almost alien, yet there was progress. I could flex my 4th toe slightly, and the tiniest twitch filled me with a joy I could barely contain. I stared at the motion for hours, each flicker a spark of hope, like watching a butterfly twitch its wings but not yet able to take flight.
Despite the heaviness in my foot, I was able to clear the floor with the help of my AF0. The first time I walked without it was a day I celebrated. I realized I could walk again, even if only cautiously, and the knowledge that I could support myself on my own feet filled me with triumph.
However, I had limited control over where my leg went. With each step, it swung unpredictably, as though trying to get away from me, testing my balance and resolve. Every movement required intense concentration, and yet each faltering step was a small victory—a reminder that my body was learning to obey again, that my mind and muscles were reconnecting, and that hope was slowly taking shape in ways I had feared lost forever.


The Frustration of Stroke Rehabilitation — One Year of Physiotherapy and Slow Progress
Rehabilitation was supposed to be the path back to myself—but some days, it felt like another battlefield I wasn’t prepared for. Physically, my body was still a stranger to me: weak, unpredictable, and painfully slow to respond. That helplessness followed me into rehab every day.
Fatigue became my constant enemy—an invisible weight that dragged through my muscles and clouded my mind. Just when I felt ready to push, it would hit without warning, stopping me mid-movement, stealing the strength I needed to complete a full set of exercises. I’d try to fight it, try to push through, but stroke fatigue is not ordinary tiredness. It was bone-deep, crushing, swallowing my energy until even lifting my arm felt like lifting a mountain. Each unfinished set left a sting of frustration, a silent whisper of failure echoing in my chest.
Rehabilitation was supposed to be the path back to myself—but some days, it felt like another battlefield I wasn’t prepared for. Physically, my body was still a stranger to me: weak, unpredictable, and painfully slow to respond. That helplessness followed me into rehab every day.
Fatigue became my constant enemy—an invisible weight that dragged through my muscles and clouded my mind. Just when I felt ready to push, it would hit without warning, stopping me mid-movement, stealing the strength I needed to complete a full set of exercises. I’d try to fight it, try to push through, but stroke fatigue is not ordinary tiredness. It was bone-deep, crushing, swallowing my energy until even lifting my arm felt like lifting a mountain. Each unfinished set left a sting of frustration, a silent whisper of failure echoing in my chest.
And then came the changes—the rotating physiotherapists, each with new methods, new styles, new exercises. Every time I adjusted, every time I built momentum, things would shift again. What my body had just learned to recognise would be replaced by something new. It felt like starting over again and again, trapped in a cycle where progress reset before I could catch my breath. I wanted consistency, familiarity, the comfort of knowing what came next—but rehab rarely offered that.
I gave everything. Full dedication. Full effort. Every ounce of strength and determination I had left. I pushed, I fought for every flicker of movement. But even with that devotion, some targets refused to budge. My body improved, yes—but never quite fast enough, never quite as much as I had hoped. There were days I left the physio room blinking back tears, wondering why my effort wasn’t enough, why recovery had to be so relentlessly slow.
And then—almost quietly—the year ended. My sessions stopped. The structure, the routine, the support that had held me together for months suddenly fell away. I felt dropped into the world again, unfinished, still fighting battles my body hadn’t fully won. Rehab didn’t end because I was “better”—it ended because the time was up. And that was a different kind of grief, one that settled heavy in my heart. I wasn’t done. My body wasn’t done. But the system had moved on.
Rehab taught me strength, resilience, and patience—but it also taught me frustration, disappointment, and the harsh reality that recovery doesn’t follow a schedule. It is messy. Uncertain. Unfair. And yet, somehow, even through the exhaustion, the inconsistency, and the heartbreak, I kept going. Because I had no choice. Because stopping was never an option.
Stroke Recovery Breakthroughs — The 45-Minute Osteopathy Correction That Changed Everything
For a year, I had been told that recovery would be slow, steady, and built through repetition. I worked relentlessly—hours of exercises, strengthening routines, corrections, stretching, gait training. I pushed my body until it shook. I did everything I was asked. Yet despite all that effort, some problems refused to move. My hip drop stayed. My foot remained stiff and painful. My knee hyperextended with every step. It felt like my body was trapped in a pattern it didn’t know how to escape.
And then, in just 45 minutes, everything changed.
I walked into the osteopathy appointment exhausted—not just physically, but emotionally. A whole year of trying had taught me not to hope too much. But within minutes, the osteopath saw what no one else had: my hip wasn’t weak—it was misaligned. My pelvis had been tilted this whole time, throwing off my entire left side—my balance, my leg swing, my knee stability, even my foot placement.

He adjusted it. A gentle, precise correction.
And suddenly, my hip drop was gone.
A pattern I couldn’t correct in twelve months of physiotherapy shifted in less than an hour. My neuro physio confirmed it. Others who saw me walk confirmed it. For the first time since the stroke, my body felt level—aligned—capable.
My foot had been a constant source of pain and confusion—cold, stiff, and difficult to weight-bear. Months of exercises hadn’t fixed it, and every step reminded me of how far I still was from normal. The same osteopath looked at my foot, paused, and said, “It’s not weak. It’s stuck.” One correction—another gentle adjustment—and the change was immediate. Warmth returned, pain lessened, and I could place weight through it without my body rebelling.
I also struggled with knee hyperextension, often called “banana leg,” where my knee bent backward as though it wanted to touch the ground. Despite months of intensive physiotherapy, switching between different physiotherapists, and giving every ounce of effort I had, nothing corrected it. Then I discovered a video demonstrating the use of an AFO (ankle-foot orthosis). I wore it continuously for six weeks, and it held my knee in the correct position, supporting my body as I moved. When I finally removed it, I realized with astonishment that my knee now sat properly beneath me, stable and aligned, where it had never been before.
These breakthroughs weren’t just physical changes—they were emotional ones. They were the first moments I felt my body wasn’t working against me anymore. Moments that reminded me recovery wasn’t linear or predictable. Moments where I finally exhaled after holding my breath for a year.
I had spent months believing I wasn’t trying hard enough. But the truth was simpler—and heartbreaking: I wasn’t misfiring. I was misaligned. And once that alignment was restored, everything else began to shift.

Resilience After Stroke — How I Rebuilt My Life and Reached 96% Recovery
The day my life changed felt like the floor had been pulled out from under me. My body, my independence, even the simplest movements became foreign and difficult. Yet, in the midst of fear, pain, and uncertainty, I discovered something remarkable: resilience isn’t a trait you either have or don’t—it’s something you awaken in yourself, moment by moment.
Resilience showed up in the smallest victories: the first time I lifted my arm without help, the first time I took a step without falling, the first night I slept knowing I was still me beneath the damage. Each tiny success was a thread, weaving together a lifeline back to myself.
Recovery demanded patience, courage, and persistence. There were days when my body refused, when my mind wavered, and when progress seemed impossible. But resilience whispered that even a fractured body and a stunned brain could learn, adapt, and grow stronger. It’s the reason I could go from collapsing at home to regaining 96% of my independence. It’s the quiet, unwavering force that reminded me: setbacks are not endings—they are the beginning of a new strength.
When traditional rehabilitation felt painfully slow, I found myself looking into alternative therapies—the ones with limited research, scattered results, success stories you could count on one hand. I knew the evidence wasn’t strong. I knew most people never saw dramatic changes. But somewhere deep inside me, I still whispered, What if I could be one of the few?
That spark of hope lit a fire in me. It made me fiercely determined to reclaim as much of my old life as humanly possible—not a partial version, not a shadow, but the closest thing to me before everything shifted. I became ruthless in my focus: cutting out anything and anyone who drained my energy, doubted my recovery, or distracted me from my mission. My life became centred around healing: physically, emotionally, and mentally.
Resilience is not about being unshakable; it’s about choosing to rise, again and again, despite fear, pain, and uncertainty. And in doing so, I found more than recovery—I found courage, hope, a deep trust in my own capacity to heal, and a fierce determination to fight for every piece of my life that stroke tried to take away.
Stroke Recovery Timeline: What to Expect
What Your Brain and Body Experience After a Stroke
A stroke doesn’t just affect one part of the brain—it disrupts how your entire body functions, rests, and recovers. Many stroke survivors experience symptoms that feel frightening, confusing, or invisible to others. Understanding what happens to the brain after a stroke can reduce anxiety, support recovery, and help survivors feel less alone.

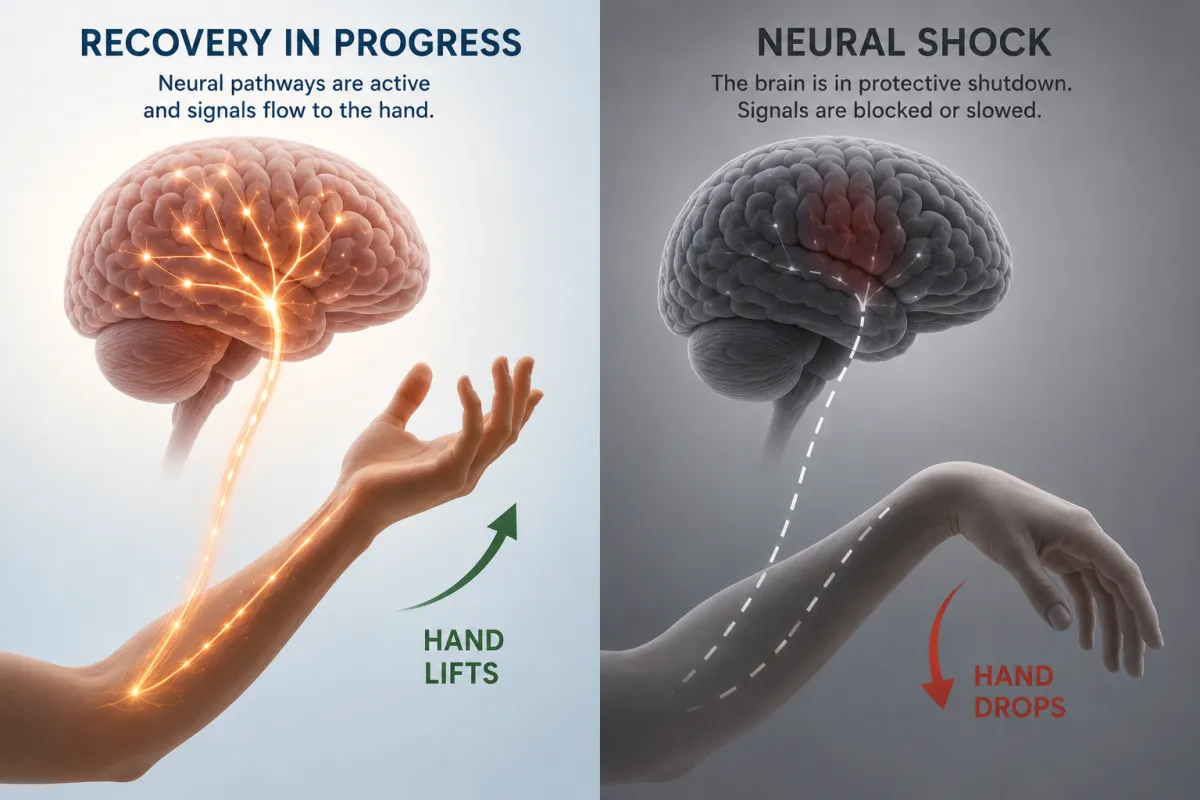
Neural Shock After Stroke — When Abilities Seem to Disappear
In the early days and weeks after a stroke, the brain often enters a protective shutdown known as neural shock. Communication inside the brain slows dramatically as it focuses on survival. This can cause sudden loss of movement, speech problems, balance issues, emotional numbness, or weakness on one side of the body.
Many survivors fear these losses are permanent. In reality, neural shock is often temporary. Functions that appear “gone” may simply be offline while the brain stabilises. As recovery progresses, abilities can return gradually—or sometimes suddenly.
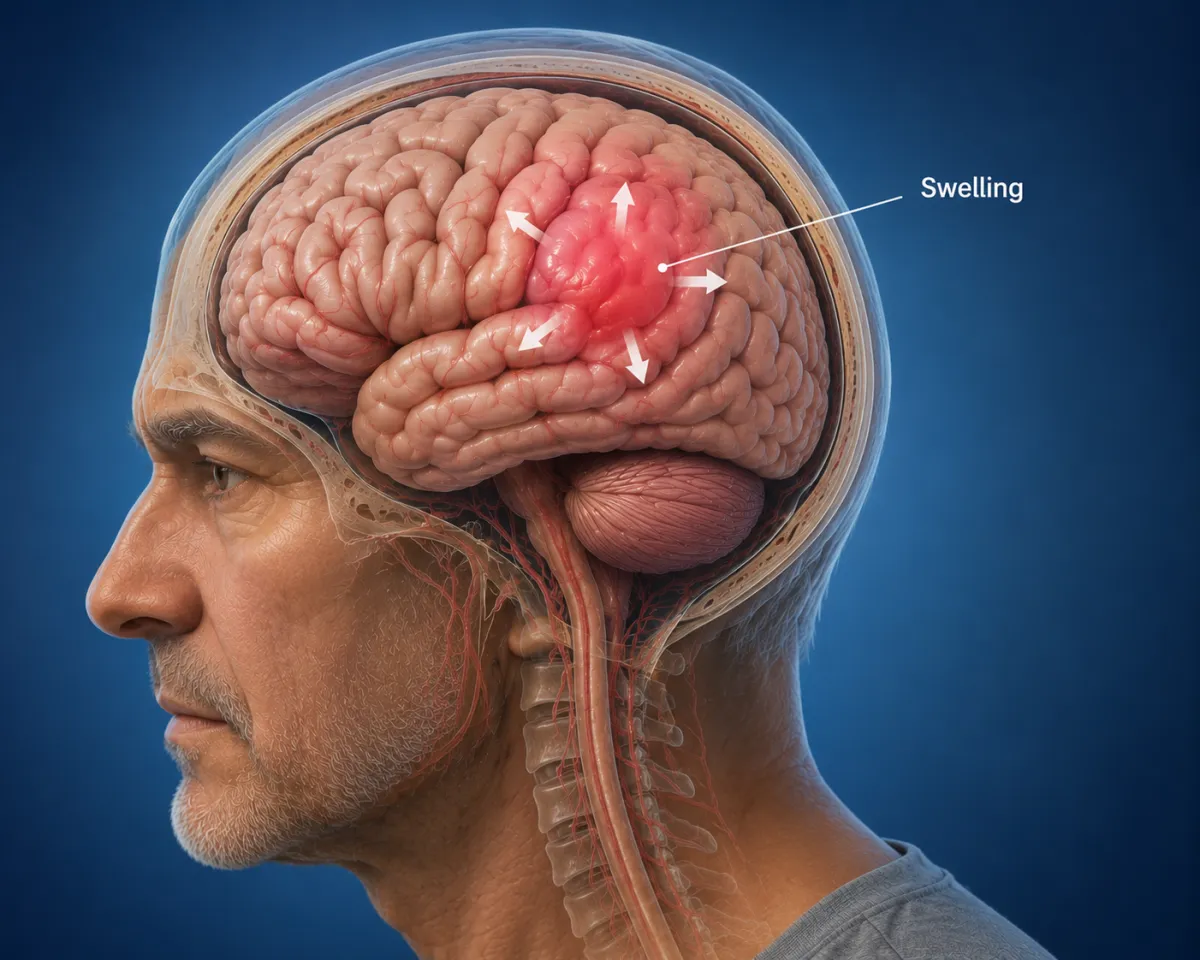
Brain Swelling After Stroke — Why Symptoms Can Look Worse at First
Brain swelling after stroke places pressure on areas responsible for movement, vision, speech, memory, and sensation. This pressure can exaggerate symptoms, making weakness, confusion, or sensory problems feel severe and permanent in the early stages.
As swelling reduces, survivors often experience improvements that were not expected. This is why early stroke prognosis is frequently inaccurate—and why recovery timelines vary so widely between individuals.

Mixed Messages Between Mind and Body After Stroke
After a stroke, the brain’s communication system can become unreliable. Messages between your thoughts and your body may arrive late, distorted, or not at all. You may know exactly what you want to do—walk, speak, lift an arm—yet your body doesn’t respond.
This disconnect is one of the most frustrating parts of stroke rehabilitation. It is not a lack of effort or motivation. It is a common stroke recovery issue that improves with repetition, rest, and time.

Sensory Overload After Stroke — When the World Feels Overwhelming
Many stroke survivors experience sensory overload after stroke. The brain struggles to filter incoming information, allowing noise, light, movement, screens, and conversations to flood in all at once.
Busy environments like supermarkets, hospitals, or family gatherings can trigger headaches, dizziness, nausea, anxiety, irritability, or emotional shutdown. These symptoms are common in stroke survivors and signal that the brain needs reduced stimulation—not more effort.

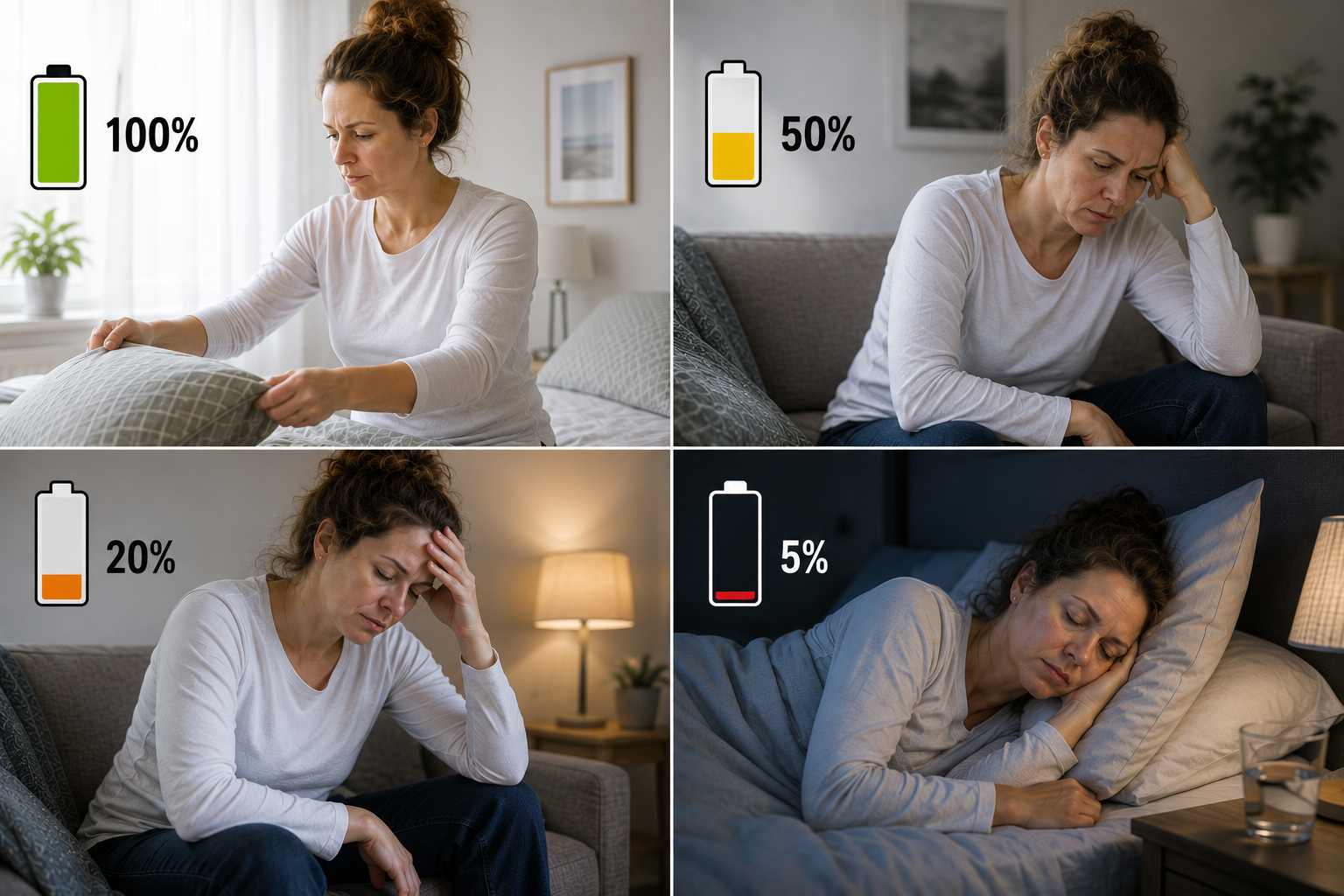
Extreme Fatigue After Stroke — The Invisible Recovery Barrier
Post-stroke fatigue is one of the most common and least understood stroke symptoms. Everyday tasks—thinking, talking, walking, concentrating—require far more energy because the brain is working harder to recover.
This fatigue can appear suddenly and feel overwhelming. It cannot be pushed through. In fact, overexertion can slow stroke recovery. Learning to pace activities and prioritise rest is a critical part of healing.

Stroke Recovery Is Not Failure — It’s Repair
If your recovery feels slow, unpredictable, or invisible, you are not doing anything wrong. Stroke recovery is rarely linear. Your brain is healing in ways you cannot see yet.
You are not broken.
You are recovering from a stroke.
The 5 Early Rehabilitation Truths ; What Doctors Often Don’t Tell You
Early stroke rehabilitation is not just about exercises and appointments. It’s about understanding how recovery actually works in the real world—something many survivors are never clearly told. These five truths can protect your recovery, reduce fear, and help you heal more effectively.

Gentle Movement After Stroke Is Safe — And Essential
Many stroke survivors are afraid to move too soon, worried they might cause damage or make things worse. In most cases, gentle movement after stroke is not only safe, it is critical. Small, supported movements help wake up communication between the brain and body, prevent stiffness, and reduce secondary complications.
Early rehabilitation is not about forcing strength—it’s about reminding the brain that movement still exists.
Repetition Matters More Than Intensity in Stroke Recovery
Stroke recovery is not about pushing harder—it’s about repeating movements consistently. Repetition after stroke teaches the brain through practice, not force. Short, frequent sessions are far more effective than exhausting workouts.
Ten slow, mindful attempts done regularly will do more for recovery than one intense session that leaves you depleted. Progress comes from consistency, not pain.


Fatigue Is Neurological — Not Personal Weakness
One of the most damaging myths in stroke recovery is that exhaustion means you’re not trying hard enough. Post-stroke fatigue is neurological. Your brain is healing, rerouting, and relearning constantly—even when you’re resting.
This fatigue is real, sudden, and overwhelming. It cannot be pushed through without setbacks. Recognising fatigue as part of recovery—not failure—protects both progress and mental health.
Rest and Pacing Are Part of Stroke Rehabilitation
Rest is not the opposite of recovery—it is a core component of it. Rest and pacing after stroke allow the brain to process learning, repair connections, and prevent overload.
Pacing means doing a little, resting before exhaustion hits, and returning later. This rhythm supports long-term recovery far better than boom-and-bust cycles of overexertion followed by setbacks.

Emotional Shifts After Stroke Are Normal
Mood changes, grief, irritability, anxiety, and emotional numbness are common in early stroke recovery. These emotional changes after stroke are not character flaws or mental weakness. They are the result of brain injury, exhaustion, identity loss, and sudden life disruption.
Emotions may feel unfamiliar or out of proportion—but they are part of healing. Support, validation, and time matter just as much as physical rehabilitation.
A Note for Stroke Survivors
Recovery is not about doing more—it’s about doing what your brain can absorb today.
Gentle movement, repetition, rest, and emotional care are not “soft options.” They are the foundation of real stroke recovery.

Neuroplasticity After Stroke: How the Brain Heals and Rewires
Neuroplasticity is your brain’s ability to create new pathways. Neuroplasticity is your brain’s natural ability to adapt, relearn, and create new routes after injury. After a stroke, when some brain areas are damaged, the brain does not simply stop—it begins finding alternative ways to get messages through.
Think of it like a road closure. When the main route is blocked, traffic doesn’t disappear; it reroutes. With practice, those new routes become faster, stronger, and more reliable.

What Neuroplasticity Really Means After Stroke
When people say “the brain rewires itself,” it can sound distant or theoretical—especially when your own body isn’t cooperating yet. In real life, brain rewiring after stroke is practical, slow, and built from ordinary moments repeated many times.
Your brain changes through repetition, intention, and consistent practice. Not through forcing outcomes. Not through pushing past exhaustion. And not through waiting until things feel easy.
Every time you try—even when nothing seems to happen—you are training your brain.
How to Activate Neuroplasticity After Stroke
Neuroplasticity isn’t something you wait for—it’s something you activate. Brain rewiring after stroke happens when the brain receives clear, repeatable, meaningful signals. The goal is not to push harder, but to practise in ways your brain can absorb and strengthen.
The strategies below are proven, practical, and accessible—even on low-energy days.

Slow, Controlled Movements After Stroke – Why Slowing Down Improves Recovery
Slowing down gives your brain time to notice what’s happening. Fast or forced movements overwhelm the brain and reduce learning. Slow, controlled movements after stroke improve accuracy, awareness, and safety.
Moving slowly helps the brain:
• Detect mistakes and correct them
• Improve coordination before strength
• Reduce fear and compensatory habits
Slow is not weakness. Slow is precision.
Even attempts that fail still matter. Each attempt sends information to the brain, helping it decide what to strengthen and what to keep.
This is why slow, focused practice is more powerful than rushing, straining, or forcing results. Neuroplasticity responds to clarity—not pressure.
Small, Consistent Movements – The Foundation of Stroke Recovery
Stroke recovery does not come from dramatic effort. It comes from small movements repeated consistently over time.
A slight finger twitch.
A controlled shift of weight.
One clearly spoken word.
These moments may feel insignificant—but to your brain, they are instructions. Each one tells the brain, this skill is still needed—find a way.
Small, consistent movements:
• Prevent overload and burnout
• Allow learning without triggering fatigue
• Give the brain time to strengthen new routes
Breakthroughs often appear suddenly, but they are built quietly—through days and weeks of effort that didn’t feel impressive at the time.


Visualization After Stroke – Training the Brain Without Movement
Your brain activates similar regions whether you physically move or vividly imagine moving. Visualization after stroke allows you to practise even when fatigue, weakness, or pain limit physical movement.
Effective visualization includes:
• Imagining the movement step by step
• Focusing on how it feels, not just how it looks
• Pairing imagery with breathing
Mental practice keeps recovery active on rest days.
Bilateral Exercises After Stroke – Reconnecting Both Sides of the Body
Bilateral exercises after stroke involve moving both sides of the body together at the same time. The stronger side acts as a guide, helping the weaker side relearn timing, rhythm, and coordination. This shared movement encourages the brain to communicate more effectively across both sides, supporting more balanced recovery.
After a stroke, many people unknowingly rely almost entirely on their stronger side. Bilateral drills gently bring the affected side back into the picture—without force or frustration.
Bilateral drills help to:
Improve symmetry and posture
Moving both sides together helps reduce leaning, collapsing, or over-compensating with the stronger side. Over time, this supports better alignment, stability, and confidence in sitting, standing, and walking.
Increase awareness of the affected side
Stroke can reduce awareness of one side of the body. Bilateral movements help “remind” the brain that the affected side still exists and matters, improving body awareness and control.
Reduce neglect and compensation patterns
When one side does all the work, the brain reinforces imbalance. Bilateral drills discourage overuse of the stronger side and help prevent habits that can slow recovery or lead to pain and strain later.
Simple, repeated bilateral actions—such as tapping both hands, marching both legs, lifting both arms together, or mirroring movements—can be surprisingly powerful. Performed slowly and consistently, they help rebuild coordination, balance, and confidence without overwhelming the brain.
Remember: the goal is cooperation between both sides of the body, not perfection. Even small, uneven movements are teaching your brain how to reconnect and rebalance.
Short, Frequent Practice – How the Brain Learns After Stroke
The brain learns best through short, frequent practice, not long sessions that lead to exhaustion. High-frequency practice strengthens learning while protecting against neurological fatigue, which is common after stroke.
Multiple short sessions each day:
Reinforce new learning by repeating clear signals to the brain
Prevent overload that can slow progress or trigger setbacks
Support sustainable recovery by allowing rest between efforts
Even five minutes, repeated often throughout the day, is far more effective than one long session done once. Consistency builds recovery—without draining the brain.


What Neuroplasticity Means for Real Stroke Recovery
Neuroplasticity is not activated by intensity—it is activated by clarity, consistency, and care. Each slow movement, imagined action, and small repetition is teaching your brain a new way forward.
You are not just exercising.
You are training your brain to heal.
Real Neuroplasticity Breakthroughs After Stroke – My Lived Recovery Examples
Hip Drop Correction and Neuroplasticity
For a full year, I worked relentlessly to correct my hip drop through exercise and strengthening. That year of repetition prepared my brain to recognise what correct alignment should feel like. When the osteopath removed the physical block through manipulation, the change was immediate. My nervous system accepted the new sensory input instantly and began to reorganise and rewire around it. The correction didn’t replace the work I had done—it unlocked it. My experience taught me that neuroplasticity isn’t just about strengthening muscles, but about giving the brain accurate information at the right time so it can finally express the movement it has been learning all along.
Knee Hyperextension — How My Brain Relearned Alignment
After my stroke, my affected knee sat behind my body when I walked and stood, creating a hyperextended position often called a “banana knee.” The underlying issue wasn’t just strength. My brain had lost an accurate sense of where my knee was in space and believed it was already correctly aligned under my body, even though it wasn’t.
Wearing an orthotic held my knee in the correct position while I walked. With every step, my brain received clear and accurate feedback about where the knee should be. Because my muscles were already stronger from therapy, my brain could use this corrected position effectively. Through neuroplasticity, this repeated feedback allowed my nervous system to update its internal map of the knee. Gradually, my brain learned to keep the knee centred during walking and standing.


Foot Drop and Neuroplasticity
After my stroke, my foot felt heavy and unresponsive. To walk, I had to lift my leg higher than normal or drag my foot behind me just to clear the ground. This wasn’t only muscle weakness—it was a breakdown in communication between my brain and foot. My brain struggled to send the right signals at the right time, and my sense of where my foot was in space was unreliable.
Strengthening exercises helped build muscle capacity, but they didn’t fully correct the problem. Walking with an AFO lifted my foot for me, allowing me to walk safely without overcompensating. With each step, my brain experienced what correct foot position and timing felt like during walking. Through neuroplasticity, this repeated, accurate feedback helped retrain my nervous system. Over time, my brain learned to activate the muscles more effectively, and my foot began to lift on its own. Eventually, I no longer needed the AFO, because my brain had relearned how to control the movement.
Emotional Effects of Stroke
Emotional Effects of Stroke: Anxiety, Depression, Identity Loss & Recovery
Learn about the emotional effects of stroke, including anxiety, depression, identity loss, fear of recurrence, and overwhelm. Evidence-based insights with reassurance for stroke survivors and carers.

Survivors Quietly Battle the Emotional Effects of Stroke
Stroke recovery affects far more than the body. Many survivors quietly experience emotional and psychological challenges that are common, evidence-based, and often misunderstood. Understanding these emotional effects of stroke can reduce fear, shame, and isolation during recovery.
Identity Loss – The Identity Crisis After Stroke No One Talks About
Many stroke survivors experience a deep sense of identity loss during recovery. Sudden changes in ability, independence, work, and family roles can shift how someone sees themselves and their place in life. Research shows that changes in self-perception after stroke are strongly linked with mood, self-esteem, and quality of life, indicating that identity disruption is a real and measurable consequence of stroke recovery.
Source: ResearchGate ➔
Identity Loss – The Identity Crisis After Stroke No One Talks About
Many stroke survivors experience a deep sense of identity loss during recovery. Sudden changes in ability, independence, work, and family roles can shift how someone sees themselves and their place in life. Research shows that changes in self-perception after stroke are strongly linked with mood, self-esteem, and quality of life, indicating that identity disruption is a real and measurable consequence of stroke recovery.
Source: PMC ➔
Anxiety After Stroke
Anxiety is a frequent emotional response after stroke and occurs significantly more often among stroke survivors than in the general population, often alongside depression. Anxiety after stroke often shows up as constant body-monitoring. Many survivors become hyper-aware of physical sensations, repeatedly checking their face, speech, or limbs and worrying that every twinge, headache, heartbeat, or moment of weakness signals something serious. This heightened vigilance can make it difficult to relax or feel safe, even in familiar environments or at rest.
Source: PMC ➔
Fear of Another Stroke
Many stroke survivors experience a fear of recurrence, which can lead to increased attention to normal bodily sensations such as fatigue, dizziness, or minor aches. While this heightened awareness can feel unsettling, it is a common and understandable response to a sudden, life-threatening event. Research shows that these anxiety responses often lessen over time with reassurance and support, and recognising them as part of recovery can reduce their impact on daily life and wellbeing.
Source: PMC ➔
Shame or Frustration During Stroke Recovery
Shame and frustration often arise when tasks that were once automatic suddenly require effort or support. These reactions are a natural response to loss of independence and change, not a reflection of personal weakness or failure. Emotional and behavioural changes after stroke — including frustration, irritability, and sadness — are well recognised and can stem from both the emotional impact of adjusting to a new reality and the neurological effects of the brain as it heals.
Source: American Stroke Association ➔
Mood Swings After Stroke
Mood swings and emotional lability are recognised psychological effects of stroke. Many survivors experience rapid or unexpected shifts in emotion, which can feel confusing or out of character. Research shows these changes are linked to altered brain function and the healing process after stroke, and they are common, temporary for many people, and not a sign of personal weakness or lack of control.
Source: PMC ➔
Depression After Stroke
Depression is one of the most common psychological effects after stroke. Research shows that around one in three stroke survivors experience depression within the first year, highlighting how widespread and understandable this response is. Depression after stroke is not a personal failure but a recognised part of recovery that deserves the same care and attention as physical rehabilitation.
Source: ScienceDirect ➔
Overwhelm During Stroke Rehabilitation
Stroke survivors often feel overwhelmed as medical appointments, therapies, information, and everyday responsibilities begin to pile up. When the brain is healing, even routine tasks can require more effort, and feeling overloaded is not a sign of weakness or failure. With time, support, and the right pacing, this sense of overwhelm can ease as confidence and capacity gradually return.
Source: Stroke Association ➔
What Helps During Stroke Recovery & Neurological Healing
Therapy (Emotional, Psychological & Relationship Support)
Working with a qualified therapist, counsellor, or neuropsychologist can be a vital part of stroke recovery and brain healing. Therapy supports emotional recovery after stroke, helps process grief and identity change, and reduces anxiety, depression, and relationship strain. For many survivors and partners, therapy provides language for experiences that feel isolating or hard to explain, improving mental health and long-term recovery outcomes.
Journaling for Stroke Recovery & Cognitive Processing
Journaling is a powerful, low-pressure tool for post-stroke recovery. Writing helps organise thoughts, manage cognitive overload, and release emotion safely. For stroke survivors experiencing memory issues, brain fog, or emotional swings, journaling can also track progress, identify triggers, and reinforce a sense of control during neurological rehabilitation.
Breathwork to Calm the Nervous System After Stroke
Gentle breathwork supports nervous system regulation, which is often disrupted after stroke or brain injury. Slow, intentional breathing can reduce neurological fatigue, manage overwhelm, and lower stress hormones. Breathwork is especially helpful during moments of anxiety, frustration, or emotional flooding and supports overall.
Speaking Honestly with Loved Ones (Communication After Stroke)
Open, honest communication after stroke reduces misunderstanding, emotional distance, and unintentional pressure. Speaking plainly about fatigue, cognitive overload, intimacy challenges, or emotional changes helps loved ones understand what support is actually needed. Honest conversations can ease relationship strain, prevent resentment, and reduce the exhausting burden of masking symptoms during stroke recovery and neurological rehabilitation.
Gentle Exposure to New Experiences (Confidence After Brain Injury)
Gradually reintroducing activities, environments, or social situations supports confidence-building after stroke without overwhelming the nervous system. Gentle exposure allows the brain to adapt at a sustainable pace, helping reduce fear, anxiety, and avoidance behaviours. This approach respects neurological fatigue, supports neuroplasticity, and encourages steady progress in post-stroke recovery.
Celebrating Micro-Wins (Motivation in Stroke Recovery)
Stroke recovery is built from small, often invisible gains. Recognising micro-wins — a task completed, a conversation managed, a moment of clarity, reduced fatigue, or improved balance — reinforces progress and motivation. Celebrating these moments helps reframe recovery as ongoing healing rather than failure, supporting mental health, resilience, and long-term neurological recovery.
Words for Those Broken Today
Stroke recovery does not erase who you are.
Symptoms, setbacks, and slow days are part of neurological healing — not a definition of your worth.
Your brain is still repairing.
Your strength is still present.
Your life after stroke is still unfolding.
But it needs you.
“You are not the shadow of what once was. Your brain is rebuilding.”
Life After Stroke: Fatigue, Work, Independence & Daily Living
Life after stroke explained. Understand post-stroke fatigue, returning to work, cognitive challenges, psychological impact, and how to rebuild independence safely and sustainably.

Understanding Life After Stroke
Recovery does not end when you leave hospital. For many stroke survivors, life after stroke is shaped by long-term neurological changes that continue quietly and unevenly long after formal care has ended. Even when walking and speech return, invisible symptoms such as cognitive fatigue, sensory overload, and emotional strain often persist and shape daily life.
Post-stroke fatigue is one of the most disabling challenges survivors face. It affects thinking, movement, emotions, stamina, independence, relationships, and the ability to work or engage socially. This fatigue can make ordinary activities such as conversation, shopping, or working feel overwhelming and disproportionate to the effort involved.
Post-stroke fatigue is neurological, not psychological. It is not laziness, weakness, or lack of resilience, but a recognised consequence of brain injury. Sustainable recovery depends on protection as much as effort, with pacing, regulation, and intentional strategies replacing the urge to push through symptoms.
Long-term recovery is most successful when survivors work with their brain rather than against it. Respecting neurological limits allows healing to continue safely over time.
Post-Stroke Fatigue: What It Is
Post-stroke fatigue is a persistent neurological exhaustion caused by brain injury. It differs significantly from ordinary tiredness and does not reliably resolve with sleep. Fatigue can fluctuate throughout the day or week and may worsen without clear warning.
Rest does not always restore energy because the brain is working harder to process information, regulate movement, and manage sensory input. Cognitive load, emotional stress, and sensory stimulation often intensify fatigue, causing activities that once felt effortless to drain energy rapidly.
Post-stroke fatigue affects concentration, attention, memory, and processing speed, frequently leading to frustration and misunderstanding. Physical stamina is also reduced, meaning survivors may tire quickly even during gentle or familiar activities. Emotional regulation can be affected, making fatigue feel heavier and harder to manage.
Despite its significant impact, post-stroke fatigue is often invisible to others, contributing to underestimation and lack of appropriate support.
Managing Stroke Fatigue Without Crashing

Pacing (Energy Conservation)
Pacing means planning activity with rest before exhaustion sets in, not after. Breaking tasks into smaller, manageable steps and spreading activity across the day or week reduces cognitive overload and prevents sudden depletion. Avoiding long, uninterrupted periods of effort protects the brain and reduces setbacks.
Alternating activity with intentional rest allows the nervous system to recover before symptoms escalate. Pacing supports neuroplastic healing and long-term functional independence. In stroke recovery, consistency consistently outperforms intensity.
Gentle Movement
Gentle movement supports circulation, balance, and emotional wellbeing without overwhelming the nervous system. Regular, low-level movement encourages brain recovery while respecting neurological limits and rebuilding stamina gradually.
Short walks, light stretching, and prescribed physiotherapy exercises are often effective starting points. Movement should leave you feeling capable rather than depleted; stopping early protects recovery and restores capacity instead of consuming it.

Energy Windows
Many stroke survivors experience brief periods of improved clarity, focus, or physical energy known as energy windows. These windows are driven by neurological rhythms rather than mindset or motivation and often become predictable once patterns are observed.
Cognitively demanding tasks, work, and social interactions are best scheduled during these periods, while lower-energy times should be protected for rest and recovery. Energy crashes signal neurological overload, not failure or lack of effort.
Avoiding the Boom–Bust Cycle
The boom–bust cycle occurs when survivors overdo activity on good days and crash afterward. This pattern is common because motivation often returns before neurological capacity, but repeated crashes slow recovery and increase fatigue sensitivity.
Sustainable recovery requires stopping before depletion, even when energy feels available. Respecting limits on good days protects progress on harder ones and supports long-term independence.


Returning to Work After Stroke
Returning to work after stroke is a gradual neurological process rather than a simple return to previous duties. Hidden symptoms such as cognitive fatigue, sensory overload, and slow processing speed often affect work capacity, even when physical recovery appears strong.
Protecting recovery while rebuilding confidence and capacity is essential. Many stroke survivors successfully return to work when the process is flexible, paced, and responsive to fluctuating symptoms.
Communicating Needs
Clear communication helps employers understand that challenges are medical rather than motivational. Explaining neurological fatigue and cognitive limits reduces misunderstanding and allows practical solutions to be implemented.
Framing needs around function, such as shorter meetings, written instructions, flexible hours, or reduced multitasking, supports sustainable performance and reduces stress.

Phased Return and Adjustments
A phased return allows the brain to adapt safely to work demands. Reduced hours, modified responsibilities, and slower timelines protect cognitive stamina and prevent burnout or relapse.
Realistic expectations often improve productivity, confidence, and long-term employability.
Managing Sensory Load
Many stroke survivors develop heightened sensitivity to noise, light, screens, and busy environments. Sensory overload can significantly worsen fatigue, headaches, and cognitive symptoms.
Quieter workspaces, reduced screen exposure, and remote or hybrid work options can substantially improve daily functioning and sustainability at work.
Cognitive Pacing at Work
Cognitive pacing balances thinking tasks with rest throughout the day. Scheduling demanding work during energy windows, limiting multitasking, and building recovery breaks into the workday protect attention as a limited neurological resource.
The Psychological Impact of Stroke
Stroke affects mental health and identity as well as physical ability. Anxiety, depression, mood changes, and grief are common, especially after discharge when support reduces.
These responses are neurological and situational — not weakness or lack of gratitude. Emotional care is an essential part of recovery.
Cognitive Fatigue, Memory & Slow Processing
Cognitive fatigue affects thinking speed, memory, attention, and emotional regulation. Survivors may experience mental shutdown after conversation, decision-making, or sensory input.
Memory difficulties, word-finding problems, and slow processing are common and often misunderstood. These are neurological symptoms and require pacing and accommodation.
Regaining Independence After Stroke
Independence after stroke grows through adaptation rather than pressure. True independence is not about returning to pre-stroke standards or doing everything alone; it is about supporting brain recovery while preserving dignity, safety, and confidence.
Redefining independence allows survivors to live well within neurological limits rather than constantly pushing against them.
Practical Tools That Support Independence
Practical tools play an important role in reducing physical strain and cognitive load after stroke. Adaptive equipment such as grab rails, shower seats, reachers, and supportive seating can improve safety and ease during daily tasks. Cognitive aids, including planners, reminder apps, alarms, and visual checklists, support memory and processing difficulties. Assistive technology such as voice-to-text software, accessibility settings, and automation tools reduces mental fatigue, while simple environmental adjustments like decluttering, labelled storage, and simplified layouts make everyday activities more manageable.
Daily Habits That Rebuild Autonomy
Daily independence is rebuilt through small, consistent habits rather than bursts of effort. Structured routines provide predictability and reduce decision fatigue, while flexibility allows rest when energy fluctuates. Breaking tasks into single steps, pacing activity, and allowing recovery time between tasks prevent overwhelm and reduce the risk of fatigue crashes. Over time, these habits strengthen functional independence and confidence.
Confidence-Building After Stroke
Confidence often lags behind physical recovery and must be rebuilt deliberately. Celebrating small wins, such as completing a task, managing an outing, or sustaining a conversation, reinforces progress and motivation. Gentle exposure to activities and social settings helps rebuild trust in the body and brain without triggering overload.
Clear communication of needs reduces anxiety and enables appropriate support, while self-compassion and patience protect emotional wellbeing and support long-term recovery.
A Final Note
Life after stroke is about learning how to live well, safely, and with dignity inside a changed brain and body. Recovery continues — and so does your capacity to rebuild a meaningful life.
Best Foods and Supplements for Stroke Recovery: Neuroplasticity, Brain Healing & Nutrition
Life after stroke explained. Understand post-stroke fatigue, returning to work, cognitive challenges, psychological impact, and how to rebuild independence safely and sustainably.
Understanding Life After Stroke
Recovery does not end when you leave hospital. For many stroke survivors, life after stroke is shaped by long-term neurological changes that continue quietly and unevenly long after formal care has ended. Even when walking and speech return, invisible symptoms such as cognitive fatigue, sensory overload, and emotional strain often persist and shape daily life.
Post-stroke fatigue is one of the most disabling challenges survivors face. It affects thinking, movement, emotions, stamina, independence, relationships, and the ability to work or engage socially. This fatigue can make ordinary activities such as conversation, shopping, or working feel overwhelming and disproportionate to the effort involved.
Post-stroke fatigue is neurological, not psychological. It is not laziness, weakness, or lack of resilience, but a recognised consequence of brain injury. Sustainable recovery depends on protection as much as effort, with pacing, regulation, and intentional strategies replacing the urge to push through symptoms.
Long-term recovery is most successful when survivors work with their brain rather than against it. Respecting neurological limits allows healing to continue safely over time.
Post-Stroke Fatigue: What It Is
Post-stroke fatigue is a persistent neurological exhaustion caused by brain injury. It differs significantly from ordinary tiredness and does not reliably resolve with sleep. Fatigue can fluctuate throughout the day or week and may worsen without clear warning.
Rest does not always restore energy because the brain is working harder to process information, regulate movement, and manage sensory input. Cognitive load, emotional stress, and sensory stimulation often intensify fatigue, causing activities that once felt effortless to drain energy rapidly.
Post-stroke fatigue affects concentration, attention, memory, and processing speed, frequently leading to frustration and misunderstanding. Physical stamina is also reduced, meaning survivors may tire quickly even during gentle or familiar activities. Emotional regulation can be affected, making fatigue feel heavier and harder to manage.
Despite its significant impact, post-stroke fatigue is often invisible to others, contributing to underestimation and lack of appropriate support.
Managing Stroke Fatigue Without Crashing

Pacing (Energy Conservation)
Pacing means planning activity with rest before exhaustion sets in, not after. Breaking tasks into smaller, manageable steps and spreading activity across the day or week reduces cognitive overload and prevents sudden depletion. Avoiding long, uninterrupted periods of effort protects the brain and reduces setbacks.
Alternating activity with intentional rest allows the nervous system to recover before symptoms escalate. Pacing supports neuroplastic healing and long-term functional independence. In stroke recovery, consistency consistently outperforms intensity.
Gentle Movement
Gentle movement supports circulation, balance, and emotional wellbeing without overwhelming the nervous system. Regular, low-level movement encourages brain recovery while respecting neurological limits and rebuilding stamina gradually.
Short walks, light stretching, and prescribed physiotherapy exercises are often effective starting points. Movement should leave you feeling capable rather than depleted; stopping early protects recovery and restores capacity instead of consuming it.
Energy Windows
Many stroke survivors experience brief periods of improved clarity, focus, or physical energy known as energy windows. These windows are driven by neurological rhythms rather than mindset or motivation and often become predictable once patterns are observed.
Cognitively demanding tasks, work, and social interactions are best scheduled during these periods, while lower-energy times should be protected for rest and recovery. Energy crashes signal neurological overload, not failure or lack of effort.
Avoiding the Boom–Bust Cycle
The boom–bust cycle occurs when survivors overdo activity on good days and crash afterward. This pattern is common because motivation often returns before neurological capacity, but repeated crashes slow recovery and increase fatigue sensitivity.
Sustainable recovery requires stopping before depletion, even when energy feels available. Respecting limits on good days protects progress on harder ones and supports long-term independence.
Returning to Work After Stroke
Returning to work after stroke is a gradual neurological process rather than a simple return to previous duties. Hidden symptoms such as cognitive fatigue, sensory overload, and slow processing speed often affect work capacity, even when physical recovery appears strong.
Protecting recovery while rebuilding confidence and capacity is essential. Many stroke survivors successfully return to work when the process is flexible, paced, and responsive to fluctuating symptoms.
Communicating Needs
Clear communication helps employers understand that challenges are medical rather than motivational. Explaining neurological fatigue and cognitive limits reduces misunderstanding and allows practical solutions to be implemented.
Framing needs around function, such as shorter meetings, written instructions, flexible hours, or reduced multitasking, supports sustainable performance and reduces stress.
Phased Return and Adjustments
A phased return allows the brain to adapt safely to work demands. Reduced hours, modified responsibilities, and slower timelines protect cognitive stamina and prevent burnout or relapse.
Realistic expectations often improve productivity, confidence, and long-term employability.
Managing Sensory Load
Many stroke survivors develop heightened sensitivity to noise, light, screens, and busy environments. Sensory overload can significantly worsen fatigue, headaches, and cognitive symptoms.
Quieter workspaces, reduced screen exposure, and remote or hybrid work options can substantially improve daily functioning and sustainability at work.
Cognitive Pacing at Work
Cognitive pacing balances thinking tasks with rest throughout the day. Scheduling demanding work during energy windows, limiting multitasking, and building recovery breaks into the workday protect attention as a limited neurological resource.
The Psychological Impact of Stroke
Stroke affects mental health and identity as well as physical ability. Anxiety, depression, mood changes, and grief are common, especially after discharge when support reduces.
These responses are neurological and situational — not weakness or lack of gratitude. Emotional care is an essential part of recovery.
Cognitive Fatigue, Memory & Slow Processing
Cognitive fatigue affects thinking speed, memory, attention, and emotional regulation. Survivors may experience mental shutdown after conversation, decision-making, or sensory input.
Memory difficulties, word-finding problems, and slow processing are common and often misunderstood. These are neurological symptoms and require pacing and accommodation.
Regaining Independence After Stroke
Independence after stroke grows through adaptation rather than pressure. True independence is not about returning to pre-stroke standards or doing everything alone; it is about supporting brain recovery while preserving dignity, safety, and confidence.
Redefining independence allows survivors to live well within neurological limits rather than constantly pushing against them.
Practical Tools That Support Independence
Practical tools play an important role in reducing physical strain and cognitive load after stroke. Adaptive equipment such as grab rails, shower seats, reachers, and supportive seating can improve safety and ease during daily tasks. Cognitive aids, including planners, reminder apps, alarms, and visual checklists, support memory and processing difficulties. Assistive technology such as voice-to-text software, accessibility settings, and automation tools reduces mental fatigue, while simple environmental adjustments like decluttering, labelled storage, and simplified layouts make everyday activities more manageable.
Daily Habits That Rebuild Autonomy
Daily independence is rebuilt through small, consistent habits rather than bursts of effort. Structured routines provide predictability and reduce decision fatigue, while flexibility allows rest when energy fluctuates. Breaking tasks into single steps, pacing activity, and allowing recovery time between tasks prevent overwhelm and reduce the risk of fatigue crashes. Over time, these habits strengthen functional independence and confidence.
Confidence-Building After Stroke
Confidence often lags behind physical recovery and must be rebuilt deliberately. Celebrating small wins, such as completing a task, managing an outing, or sustaining a conversation, reinforces progress and motivation. Gentle exposure to activities and social settings helps rebuild trust in the body and brain without triggering overload.
Clear communication of needs reduces anxiety and enables appropriate support, while self-compassion and patience protect emotional wellbeing and support long-term recovery.
A Final Note
Life after stroke is about learning how to live well, safely, and with dignity inside a changed brain and body. Recovery continues — and so does your capacity to rebuild a meaningful life.
Best Foods and Supplements for Stroke Recovery: Neuroplasticity, Brain Healing & Nutrition
Foods That Support Brain Recovery After Stroke
After a stroke, the brain has to work much harder than before. Learning, concentrating, moving, and even resting can take more effort. Recovery happens mainly through therapy, practice, rest, and pacing — but food can help support the brain while this work is happening.
Food does not cause recovery on its own. It cannot replace rehabilitation or time. But the right foods can help support brain health, reduce stress on the brain, and provide steady energy during recovery.
The foods below are commonly talked about because they support overall brain health and may help the brain cope better with the demands of recovery.
Blueberries: Supporting Memory and Thinking
Blueberries contain natural compounds that help protect brain cells from stress and damage. After a stroke, the brain is more sensitive and can become tired or overloaded easily.
People often include blueberries because they are linked with better memory, learning, and communication between brain cells. This can be helpful for survivors who experience brain fog, mental tiredness, or difficulty concentrating.
Salmon: Supporting Brain Communication
Spinach and other leafy greens contain vitamins and minerals that help support the brain and blood flow. Good blood flow is important for keeping the brain nourished and functioning well.
Including leafy greens in meals is often linked with better attention, focus, and slower memory decline. This can help reduce mental strain during everyday activities.
Eggs: Supporting Memory and Muscle Control
Eggs contain a nutrient that helps the brain make chemicals needed for memory, attention, and muscle control.
This can be helpful after a stroke, especially if you notice forgetfulness, difficulty focusing, or problems coordinating movement. Eggs are also easy to prepare and can be a practical option when energy is low.
Avocado: Supporting Blood Flow and Energy
Avocados contain healthy fats that support good blood flow, including to the brain. After a stroke, the brain benefits from steady circulation and consistent energy.
Avocados also contain nutrients that support both heart and brain health. They can help support stamina and reduce strain on the brain during recovery.
Walnuts: Supporting Brain Protection
Walnuts contain healthy fats and natural plant compounds that help protect brain cells.
They are often included in recovery diets because they support thinking, learning, and memory. Walnuts are a simple way to add brain-supportive nutrients without major dietary changes.
How Food Fits Into Stroke Recovery
Food helps support recovery by:
reducing stress on the brain
helping protect brain cells
supporting steady energy
supporting thinking and concentration
However, food alone does not drive recovery.
Recovery mainly comes from:
rehabilitation and practice
rest and sleep
pacing and managing fatigue
emotional support and regulation
Food works best when it supports these foundations, not when it is treated as a cure.
Key message: Eating for recovery is not about strict diets or doing everything perfectly. It is about regular nourishment and choosing foods that support your brain over time. Food supports recovery. Practice builds it. Time allows it.
Supplements People Often Ask About After Stroke
(Based on survivor experience — not medical advice)
Many stroke survivors ask about supplements, especially when they feel very tired, low in energy, or mentally exhausted.
It’s important to know that many people after stroke take medications such as blood thinners or blood pressure drugs. Supplements can sometimes interfere with these medications. Always talk to a doctor, GP, or pharmacist before starting any supplement.
The supplements below are commonly talked about in recovery communities, but they are not treatments and do not replace medical care.
Omega-3 Supplements
Omega-3 supplements are often discussed because they support brain cell health and communication.
Some survivors feel they help with thinking clarity or mood stability. Others notice no difference. Responses vary, and medical advice is important before using them.
Magnesium
Magnesium is often mentioned by people dealing with muscle tightness, poor sleep, or nervous system overload.
Some survivors report better sleep or muscle comfort, especially during demanding rehabilitation periods. Effects vary, and magnesium may not be suitable for everyone.
B-Complex Vitamins
B-vitamins are important for nerve health and energy levels.
People often ask about them when dealing with fatigue, brain fog, or low mental energy. Blood tests are sometimes needed to check whether supplementation is appropriate.
Vitamin D
Vitamin D is commonly discussed because it supports bones, muscles, mood, and balance.
Low levels are common after stroke, especially if time outdoors is limited. Doctors sometimes recommend checking levels before supplementing.
CoQ10
CoQ10 is linked to how the body produces energy. Some survivors explore it when dealing with long-lasting fatigue or low stamina.
Research is still ongoing, and effects differ between individuals. Medical advice is important before trying it.
Important Reminder About Supplements
Supplements may support the body, but they do not create recovery. Stroke recovery comes from practice, rest, pacing, emotional care, and time.
What helps one person may not help another. Recovery is individual, and safety always comes first. If you are unsure about supplements, speak with your neurologist, GP, or rehabilitation specialist before starting anything new.
Discover the best foods and commonly discussed supplements for stroke recovery. Learn how nutrition supports neuroplasticity, brain healing, energy, and long-term neurological rehabilitation.
Stay Updated
Get the Latest News Delivered to Your Inbox
Never Miss an Update – Subscribe for Fresh News & Insights!

Alisia Gayle is a stroke survivor, author, and advocate whose life was transformed in a single, ordinary day.
COMPANY
Quick links
Copyright 2026. Alisia Gayle | Stroke Recovery Through Lived Experience. All Rights Reserved.